
Blog
LL-37 Peptide Benefits: The Antimicrobial Peptide LL37 for Lyme and Chronic Infections

If you have been sick on repeat, you start to question everything. Was it a tick bite, a sinus issue that never cleared, or a virus that keeps waking up?
LL-37 shows up in these searches because it is part of the body’s own first-line defense, and people wonder if that same signal can be used on purpose when symptoms drag on.
Start here: chronic symptoms are real, but the cause can differ
Some people have a clear infection that never fully clears, while others clear the germ yet keep fatigue, pain, and brain fog, and that splits what testing and care make sense next. That is why one person may need antibiotics, while another may need rehab and sleep work.
Lyme is a good example. Many people get better after standard treatment, yet a subset keeps fatigue, pain, or brain fog for months.
If Lyme is on your mind, these pages can help you sort the basics before you chase new tools.
Infection, post-infection, or both?
These labels are not just words. They shift what tests make sense, and what tools are likely to move the needle.
More likely ongoing infection
- Fevers that keep returning
- New rashes, swollen joints, or nerve signs after a known exposure
- Clear imaging or lab clues that keep pointing to infection
More likely post-infection pattern
- Symptoms that stay, but without clear signs of active infection
- Wide symptom spread that shifts day to day
- A pattern that tracks with sleep loss and stress load
For long-lasting symptoms after Lyme treatment, major guidelines advise against more antibiotics when there is no objective sign of active infection.
Why do people look beyond antibiotics?
Antibiotics can save lives. They can also fall short when microbes hide in tissues, form biofilms, or when symptoms are no longer driven by live bacteria.
There is also the real issue of side effects and gut disruption from long courses. That drives a lot of people to search for “chronic infection alternative treatments,” even if they still plan to use standard care.
A useful place to start is a map of common “stuck points” seen with long-lasting infection symptoms.
A simple immune primer: what matters for LL-37
Your immune defenses have two big arms. One is fast and broad (innate). The other is slower but more specific (adaptive).
LL-37 sits closer to innate defense. It is made at barrier sites and by immune cells that act early, before antibodies even show up.
If you want the broader peptide context first, start with peptide basics.
Stress can shift immune tone
Stress is not “all in your head.” It shifts sleep, blood sugar, and cortisol, and those shifts can affect how you react to germs and inflammation.
What is LL-37?
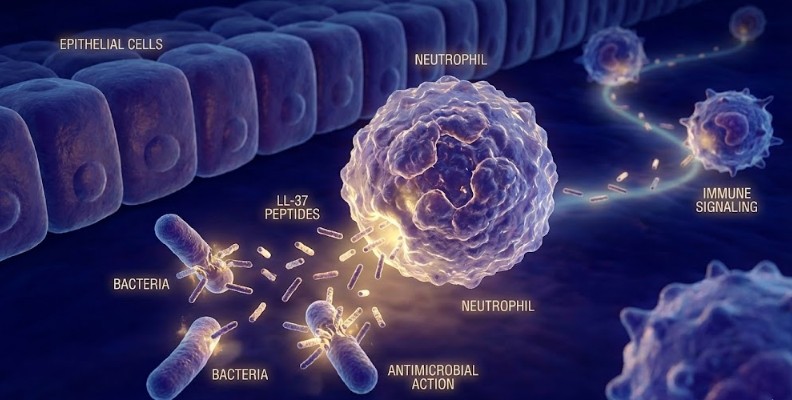
LL-37 is the active fragment of a human protein called hCAP18. It is the only human cathelicidin, and it is released by cells like neutrophils and epithelial cells when there is tissue stress.
People call it an “antimicrobial peptide,” but that label is only part of the story. LL-37 can also act like a signal that calls in immune cells and shifts how they behave.
Where LL-37 is made, and why location matters
LL-37 is stored in immune cells that patrol the blood. It is also made by lining cells in places where germs first land, like skin, airways, and the gut.
This matters because “infection” is not one setting. Salt, pH, mucus, and tissue damage can all shift how a peptide behaves once it is in the body.
Vitamin D and LL-37: the link people mention
Vitamin D can switch on the CAMP gene in certain cells, which is one way the body makes more LL-37.
That does not mean vitamin D alone fixes chronic infections. It does mean a simple lab check can be a smart early move, since low vitamin D is common and easy to correct with a clinician.
How LL-37 acts in the body
LL-37 tends to get described in three lanes: microbe pressure, biofilm effects, and immune signaling. Each lane has limits.
Here is the headline: LL-37 is not a single-action drug, and that is why it gets attention in long-lasting infection patterns.
1) Microbe pressure is real, but not equal across germs
LL-37 can damage microbial membranes in lab work. It has activity against many bacteria, fungi, and some viruses, but the dose needed varies a lot.
For Borrelia species in lab testing, LL-37 showed weak activity, with very high concentrations needed to stop motility.
That means “LL-37 kills Lyme” is not a safe claim. Any use in Lyme care is more likely to be indirect or tied to broader immune signaling.
2) Biofilms: the sticky layer that can make treatment harder
A biofilm is a slimy matrix that microbes use to stick to surfaces and to each other. Inside it, microbes can be less sensitive to antibiotics and to immune attack.
In a lab model, LL-37 blocked biofilm formation by Pseudomonas at low concentrations, even below levels needed to stop growth.
Biofilms are not just “slime.” They are a mesh of sugars, proteins, and DNA that lets microbes stick, share resources, and hide from both drugs and immune cells.
Inside a biofilm, microbes can slow down. Many antibiotics work best on fast-growing germs, so slow or dormant cells can survive a course and then flare later.
This is why some people feel better during a round of antibiotics, then slide back after it ends. The medication may lower free-floating germs, while the protected pocket stays.
It also explains why chronic sinusitis, dental infections, and device-related infections can act so stubborn. In those cases, the fix is often part mechanical, part medical, and not just “try another pill.”
This is one reason LL-37 is discussed in stubborn sinus and airway issues, where biofilms can play a part.
If sinus flares are part of your story, you may also want to read mold signs since indoor exposure and sinus symptoms often overlap.
3) Immune signaling: where LL-37 can cut both ways
LL-37 can call immune cells to a site and shift cytokine signals, which are small messenger proteins that tell immune cells what to do. In some contexts, that may help clear a stubborn problem.
In other contexts, too much LL-37 signaling may fan inflammation. Reviews discuss LL-37’s part in autoimmune skin disease, where LL-37 can form complexes with self-DNA and trigger immune activation.
This is why screening matters. An immune “push” can be the wrong move for some people.
LL-37 and chronic infections: where it tends to come up
LL-37 usually enters the chat when someone has repeated infections or a chronic pattern that never feels fully calm.
Below are common buckets where LL-37 gets mentioned, with a short list of other checks.
Chronic Lyme symptoms
Some people have clear Lyme that was treated, yet symptoms keep going. Other people never had a clear early rash, so the picture stays fuzzy.
Public health agencies use the term PTLDS for prolonged symptoms after treated Lyme, and they discourage “chronic Lyme disease” as a blanket label, since ongoing symptoms are not always driven by ongoing infection.
Chronic sinusitis and biofilm patterns
Some people get “sinus infections” that come back every month. Others have congestion, pressure, and post-nasal drip with no clear fever.
LL-37 is present in the nasal lining, and levels can rise in inflamed nasal tissue.
If you keep getting sick, it can be useful to zoom out and look at triggers like sleep, reflux, mold exposure, and allergy patterns.
Viral flares and “always run down” patterns
Some viruses can go latent, then flare again when sleep and stress are off. EBV is one common example.
Gut-driven inflammation that looks like infection
Bloating, loose stools, and skin flares can make people feel “infected,” even when the driver is gut barrier irritation and immune activation.
Lyme and long symptoms: a clearer map
Lyme starts with a tick bite that transmits Borrelia bacteria. Early signs can include a spreading rash, fever, body aches, and swollen nodes, yet some people never see a classic bullseye.
Testing can be confusing because most routine tests look for antibodies. If you test too early, antibodies may not be there yet, even if you feel sick.
For early Lyme with the classic rash, guidelines allow a clinical diagnosis without lab testing.
For other presentations, guidelines lean on antibody testing and symptom patterns.
Treatment also depends on the form of the disease. Early disease is often treated with oral antibiotics for a short course, while nerve or heart involvement can call for a longer course and sometimes IV therapy.
What “persistent symptoms” can mean after treatment
Some people experience fatigue, pain, sleep issues, or brain fog after treatment. That pattern is often called PTLDS, and the cause is not fully settled.
This is where the plan may shift from “kill a germ” to “calm inflammation, rebuild sleep, and rehab function,” while still watching for objective signs of active disease.
Coinfections and look-alike infections
In some regions, ticks can carry more than one germ. Coinfections can shift symptom patterns and lab clues, like anemia or low platelets.
A separate issue is that mold exposure, chronic viral reactivation, and gut inflammation can mimic parts of the Lyme symptom cluster.
Where LL-37 fits in Lyme circles
LL-37 does not look like a clean “anti-Borrelia drug” in lab testing.
So when LL-37 is used in Lyme circles, the goal is usually broader: pressure on mixed microbes, biofilm effects, and immune signaling that may help the body reset after repeated hits.
A quick table: LL-37 vs two other immune peptides
Many people look at LL-37 next to other immune peptides. The three below get compared often because they show up in similar conversations.
| Peptide | Main idea | Where it often shows up | Main caution |
|---|---|---|---|
| LL-37 | cathelicidin signal + antimicrobial peptide | recurrent infections, stubborn biofilm patterns, Lyme circles | may raise inflammation in some immune patterns |
| Thymosin Alpha-1 | thymus-linked immune modulator | chronic viral patterns, immune suppression patterns | not a DIY move if you are on immune drugs |
| BPC-157 | tissue repair signal | gut lining stress, tendon issues, recovery | product purity and long-term data gaps |
Who should be careful with LL-37?
LL-37 is not a casual add-on. If you have a history of autoimmune disease, psoriasis, lupus, or unexplained inflammatory flares, use extra care.
LL-37 is discussed in autoimmune skin disease because it can drive immune activation in certain settings. That is a signal to slow down and get screened first.
Also, use care if you are pregnant, nursing, or have a transplant history, since immune shifts carry extra risk.
Practical safety: why sterile technique matters
LL-37 is often used as an injectable peptide, which changes the safety picture. Anything injected can irritate tissue, and any lapse in cleanliness can raise infection risk.
Watch for redness that spreads, warmth, pus, fever, or a streak moving away from the injection spot. Those signs need fast medical care.
Also watch for “immune flare” symptoms that feel out of proportion, like new joint swelling, hives, chest tightness, or severe fatigue that hits within hours.
If you are on immune-suppressing drugs, have a transplant history, or are pregnant or nursing, do not start LL-37 on your own. Talk with the clinician who manages your meds so timing, risks, and lab follow-up are clear.
What to test and rule out before you chase LL-37

A peptide cannot fix what you have not named. Many “infection” symptoms are driven by sleep loss, anemia, thyroid issues, hormone swings, or mold exposure.
This checklist is meant to save you time and money. It also lowers the odds that you treat the wrong thing.
Four screens that can alter the plan fast
- Sleep apnea risk if you snore, wake unrefreshed, or have morning headaches
- Iron and B12 status if fatigue and shortness of breath show up
- Thyroid labs, if cold intolerance, hair loss, or constipation show up
- Blood sugar swings if you crash mid-afternoon or wake at 3 a.m.
Infection workups that often get missed
Lyme itself is not the only tick-borne problem. In some regions, co-infections like babesiosis or anaplasmosis can shift symptoms and lab patterns.
People also miss chronic dental infections, chronic sinus biofilms, and urinary infections that keep recurring due to an anatomic issue.
A 30-day way to spot patterns before you add a new therapy
When symptoms are noisy, memory lies. A simple log can show patterns you missed, like a short-sleep week, a travel flare, or a food trigger that repeats.
Keep it simple. One page per week is enough, and you only need a few data points.
Track these each day
- Sleep time and wake time
- A 0–10 score for fatigue, pain, and brain fog
- Temperature if you feel “flu-ish”
- Bowel pattern (constipation, loose stool, or normal)
- Any alcohol, late sugar, or late workouts
- Stress load in one word (calm, tense, overloaded)
After two weeks, look for repeats. If flares track with sleep debt, you may get more from sleep work than from another antimicrobial.
If flares track with meals, start with gut basics and labs before you reach for another peptide.
Red flags that should not wait
Call urgent care or go to an ER if you have chest pain, fainting, a stiff neck with fever, sudden weakness on one side, or a new rash with trouble breathing.
For Lyme in particular, new severe headaches, facial droop, heart palpitations with dizziness, or a swollen joint that is hot and large should be checked fast.
A clinician-led protocol: where LL-37 fits, and where it does not
In clinic settings, LL-37 is usually treated as one tool in a wider plan. The plan may still include antibiotics, antifungals, or antivirals when they are needed.
Think of LL-37 as a possible adjunct. It is not a replacement for diagnosis, and it is not a reason to stop standard care on your own.
Why stacking random “infection tools” can backfire
If you pile on antimicrobials without a plan, you can flare inflammation, disrupt the gut, and feel worse.
It can also blur the picture. When five things shift at once, you cannot tell what caused the shift.
A safer rhythm is one move at a time, tracked with symptoms, sleep, and basic labs.
Lifestyle levers that set immune tone

Peptides get attention, but daily habits still set your immune tone. When the basics are off, many therapies feel weaker.
Here are three levers that show up in almost every chronic infection story.
Sleep as immune training
Short sleep can raise inflammation and lower antiviral defenses. One bad night is annoying, but weeks of short nights can alter how you react to everyday germs.
Blood sugar swings
A big sugar spike late can lead to a 2 a.m. wake with a racing mind. That wake can then raise next-day cravings, and the loop repeats.
Simple meal timing, protein at breakfast, and less alcohol often break this loop within two weeks.
Stress load and recovery time
When stress stays high, your body can stay in a low-grade fight mode. That can show up as shallow sleep, gut flares, and more frequent colds.
Common questions about LL-37 for Lyme and chronic infections
Is LL-37 an antibiotic?
No. It is a peptide that acts like a host defense signal and has antimicrobial effects in lab models, but it is not a standard antibiotic drug.
Does LL-37 “kill Lyme”?
In lab testing against Borrelia strains, LL-37 shows weak direct activity at very high concentrations.
Any real-world use for Lyme circles is usually framed as adjunctive, not as a stand-alone “Lyme killer.”
Why do some people feel worse on LL-37?
One possibility is immune activation. LL-37 can raise cytokine signals, and in some immune patterns that can feel like a flare.
Another possibility is product purity, dosing errors, or using it in a body already in a high-inflammatory state.
Is LL-37 the same thing as vitamin D?
No. Vitamin D is a nutrient hormone that can affect LL-37 gene expression in some tissues, but LL-37 itself is a peptide fragment with its own actions.
Can LL-37 be used with antibiotics?
In lab work, antimicrobial peptides can interact with antibiotics and biofilms in useful ways.
In real care, the safest rule is simple: do not mix therapies without a clinician who can track side effects and labs.
What symptoms make Lyme more likely?
Early Lyme often starts with a rash, fever, and body aches, but not everyone gets the classic bullseye rash. Later signs can include joint swelling, nerve pain, or heart rhythm issues.
A lab test is not perfect, so timing and symptoms matter.
What symptoms make “post-infection” more likely?
If symptoms stay for months after standard Lyme treatment, with no objective sign of ongoing infection, that pattern is often called PTLDS.
That does not make symptoms less real. It just shifts the plan toward rehab, sleep, work, pain care, and immune calming.
Should I use LL-37 if I have psoriasis or lupus?
Use extra care. LL-37 is linked with immune activation in some autoimmune skin disease settings, and that is a signal to slow down and get screened first.
What is a safer first move if I keep getting sick?
Start with basics you can measure: sleep, iron, vitamin D status, glucose balance, and stress load.
Your next step can be calmer and clearer
When you have lived with long symptoms, it is easy to chase the newest tool. A better move is a plan that starts with the basics, rules out red flags, and then adds one therapy at a time.
Bring your symptom log and recent labs to the visit so choices feel grounded, not random.
If you feel stuck, a fresh set of eyes can spot repeat triggers and keep you from cycling through one new tool after another.
If you want a clinician-led plan that may include LL-37, you can start by booking or learn more about peptide therapy.