
Blog
How Peptide Therapy for Skin Rejuvenation Actually Works — And Which Peptides Do What

Most anti-aging skincare works on the surface. It moisturizes, reflects light, temporarily fills fine lines, or removes dead skin cells. None of that changes what’s happening in the dermal layer where collagen is produced, where cells divide, and where the structural decisions that determine skin firmness, texture, and healing speed are made. Peptide therapy for skin rejuvenation addresses aging at that deeper level — by giving cells the signaling molecules they need to behave like younger tissue.
The shift from surface treatments to cellular ones reflects a better understanding of why skin ages. Collagen production peaks in your mid-twenties and declines roughly 1% per year after that. Dermal fibroblast activity slows. NAD+ levels drop across skin tissue. Telomere length shortens with each cell division, eventually pushing cells into senescence. These are measurable biological changes, and they respond to specific biological inputs, which is what therapeutic peptides provide.
This post covers how peptides work as cellular signals, why injectable delivery outperforms topical for most applications, which specific peptides are used for skin and collagen goals, and how to structure a protocol.
⚠ Disclaimer: LIVV Peptides products are for research use only and are not intended for human consumption. LIVV Peptides is a chemical supplier, not a compounding pharmacy. All content here is informational. Consult a licensed medical provider before beginning any peptide protocol.
What Peptides Are and Why They Matter for Skin Rejuvenation
Peptides are short chains of amino acids — the same building blocks that make up proteins. In biological systems, they function as signaling molecules: the body uses them to tell specific cells to do specific things. A peptide that triggers collagen synthesis signals dermal fibroblasts differently than one that activates tissue repair pathways or stimulates growth hormone release. The signal determines the response.
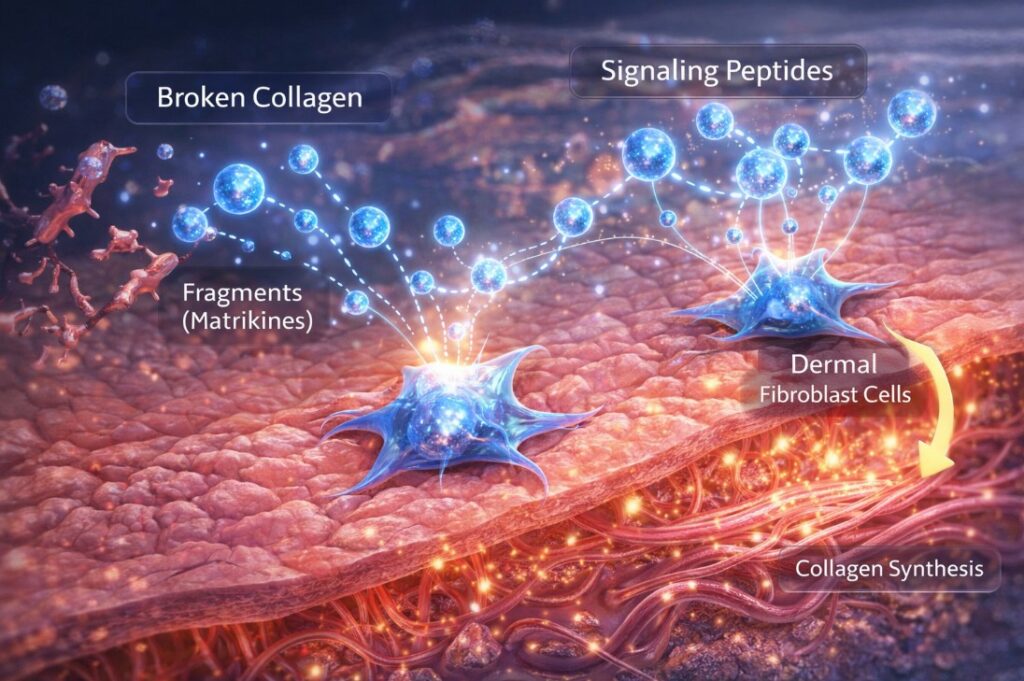
Your skin produces signaling peptides naturally. When collagen breaks down, fragments of it — called matrikines — bind to fibroblast receptors and trigger new collagen production as a repair signal. This feedback loop is how healthy young skin maintains its structure. The problem is that this system becomes less responsive with age: fewer receptors, lower baseline activity, and a reduction in the overall peptide signaling environment that keeps skin in a regenerative state.
The peptides used therapeutically either mimic these natural signals or produce effects that natural peptide production can’t reliably achieve at the needed levels. Some directly stimulate growth hormone release, which increases collagen density across the dermis. Others act specifically on wound repair pathways, or on the cellular aging mechanisms that determine how long skin cells continue to function before entering senescence. Understanding which peptide does which helps in choosing the right protocol for a specific goal.
Natural peptide production begins declining in most people by their early thirties. The result — slower skin cell turnover, reduced collagen synthesis, weaker repair response to sun damage and environmental stress — is what most people notice as the first signs of aging. Protecting and rebuilding collagen requires addressing those upstream signaling deficits, not just the collagen loss itself.
Topical vs. Injectable Peptide Therapy: Why Delivery Method Changes Everything
The skincare industry has used topical peptides for years — copper peptides, palmitoyl tripeptide-1, acetyl hexapeptide-3. These have a place, but their effect is constrained by one fundamental problem: most peptides don’t cross the skin barrier in meaningful amounts. The stratum corneum — the outermost layer of skin — is specifically designed to keep large molecules out. Peptides above a certain molecular weight simply don’t penetrate to the dermis, where fibroblasts and collagen production happen.
Topical peptides that do absorb tend to produce modest results because the concentration reaching the target tissue is a fraction of what was applied. Manufacturers compensate by using peptide fragments or lipid-conjugated peptides that absorb more readily, but these are workarounds, not solutions. The dose that reaches fibroblasts is still low compared to what systemic delivery achieves.
Injectable peptides administered subcutaneously enter the bloodstream directly and reach target tissues at therapeutic concentrations. For peptides that work systemically — like growth hormone secretagogues that act on the pituitary, or repair peptides like BPC-157 that work through systemic circulation — this is the only delivery method that reliably produces the expected effect. Results from injectable protocols are typically visible within 4 to 8 weeks with consistent use, and the changes reflect actual shifts in collagen density, skin thickness, and cellular repair activity rather than surface conditioning.
There are cases where topical delivery makes sense — GHK-Cu copper peptide is one example where topical application has reasonable evidence for collagen stimulation at the skin surface. But for the major therapeutic peptides used in aesthetic and longevity protocols, injectable delivery is the baseline for reliable results.
The Key Peptides for Skin Rejuvenation and Collagen Production
BPC-157: Tissue Repair, Collagen Deposition, and Blood Vessel Formation
BPC-157 (Body Protection Compound 157) is a 15-amino acid peptide derived from a naturally occurring sequence in gastric juice. Its primary application in skin aesthetics is wound repair, inflammation reduction, and acceleration of collagen remodeling. A study published in Drug Design, Development and Therapy demonstrated that topical BPC-157 accelerated wound closure in an alkali burn model, with histological analysis showing superior granulation tissue formation, re-epithelialization, dermal remodeling, and significantly higher collagen deposition compared to controls. The mechanism involves upregulation of VEGF expression — a key growth factor in new blood vessel formation — and activation of ERK1/2 signaling pathways that drive cell proliferation, migration, and angiogenesis.
For aesthetic applications, BPC-157 is used for post-procedure skin repair — accelerating recovery after laser treatments, microneedling, or PRP procedures — and for reducing the appearance of scars by improving collagen organization in the healing tissue. It also has anti-inflammatory effects that reduce the redness and swelling associated with both aesthetic procedures and chronic skin inflammation.
Epithalon: Cellular Aging, Telomere Support, and Skin Renewal
Epithalon (also written Epitalon) is a synthetic tetrapeptide with the sequence Ala-Glu-Asp-Gly, originally identified from pineal gland extracts. Its primary relevance to skin aging is its effect on telomere length. Telomeres are the protective caps at the ends of chromosomes that shorten with each cell division — critically short telomeres trigger cellular senescence, the state in which cells stop dividing and start secreting inflammatory signals that degrade surrounding tissue. A 2025 study published in Biogerontology demonstrated dose-dependent telomere length extension in normal human cells through upregulation of hTERT (the telomerase catalytic subunit) and telomerase enzyme activity — meaning Epithalon appears to reactivate the cellular machinery that maintains telomere length rather than just slowing its shortening.
For skin specifically, this matters because the accumulation of senescent fibroblasts in aging dermis is one of the primary drivers of collagen loss. Senescent cells stop producing collagen, begin secreting enzymes that degrade existing collagen and elastin, and create a local inflammatory environment that accelerates surrounding tissue aging. Interventions that slow or reduce cellular senescence — including telomere maintenance — address this mechanism at its source. Epithalon also appears to restore melatonin regulation through its effect on the pineal gland, which has downstream effects on overnight skin repair and oxidative stress recovery.
CJC-1295 and Ipamorelin: Growth Hormone Release and Dermal Collagen
CJC-1295 and Ipamorelin are typically used together as a growth hormone secretagogue stack. CJC-1295 is a modified GHRH (growth hormone-releasing hormone) analog that extends the half-life of GH release, while Ipamorelin is a selective GH secretagogue that stimulates pituitary release without significantly affecting cortisol or prolactin levels. The combination produces a sustained, physiologically timed increase in growth hormone — typically administered at night to align with the natural GH pulse during sleep. A more detailed breakdown of how this combination works is covered in the peptide therapy anti-aging overview on the LIVV blog.
For skin, growth hormone has direct effects on dermal structure. GH stimulates IGF-1 production in the liver and locally in skin tissue, which in turn drives fibroblast proliferation and collagen synthesis. Clinical data on GH-deficient adults consistently show thinner, less elastic skin as a feature of deficiency, with improvements in skin thickness and collagen density following GH replacement. While the GH increase from CJC-1295/Ipamorelin is more modest than pharmaceutical GH replacement, it operates through the same pathway and avoids the side effect profile associated with exogenous GH administration.
The expected skin-related changes from a consistent CJC-1295/Ipamorelin protocol include increased skin thickness, firmer texture, improved elasticity, and a more even surface appearance. These changes typically become noticeable within 8 to 12 weeks and continue to develop over the course of a full 3 to 4 month cycle.
Tesamorelin: Structural Support and Skin Elasticity
Tesamorelin is a synthetic form of GHRH — growth hormone-releasing hormone — with a longer half-life than the naturally occurring molecule. It’s been studied more extensively than most growth hormone secretagogues because it received FDA approval for visceral fat reduction in HIV-associated lipodystrophy, which means it has a well-documented safety and efficacy profile in humans. The mechanism is the same as CJC-1295: stimulation of pituitary GH release, leading to increased IGF-1 and downstream effects on collagen-producing cells in the dermis.
Tesamorelin is used in skin protocols, particularly for facial structural support — the kind of volume and firmness that reflects healthy dermal thickness rather than surface texture. People who notice progressive hollowing of the mid-face, reduced definition along the jawline, or generalized skin laxity that isn’t responding to topical interventions tend to see better outcomes with GH-releasing peptides like Tesamorelin than with surface-level aesthetics alone.
TB-500 (Thymosin Beta-4): Wound Repair, Scar Reduction, and Collagen Organization
TB-500 is a synthetic version of Thymosin Beta-4, a naturally occurring peptide found in high concentrations at injury sites throughout the body. Its primary function is in tissue repair: it promotes actin polymerization (required for cell movement), upregulates anti-inflammatory proteins, and stimulates the migration of keratinocytes and endothelial cells that are needed to close and repair damaged tissue. For aesthetic applications, TB-500’s main use is in improving scar appearance, accelerating healing after procedures, and supporting the collagen remodeling phase that determines whether a healed wound leaves smooth or irregular scar tissue.
TB-500 is often paired with BPC-157 in recovery protocols because the two peptides act through complementary mechanisms — BPC-157 primarily through growth factor upregulation and angiogenesis, TB-500 through cell migration and actin dynamics. Together, they address more stages of the repair process than either does alone. For post-procedure skin recovery, this combination is particularly well-suited.
NAD+ and Skin: Cellular Energy, DNA Repair, and Collagen Maintenance
NAD+ (nicotinamide adenine dinucleotide) is not a peptide in the conventional sense, but it’s included in peptide therapy protocols for skin rejuvenation because it addresses one of the most upstream causes of skin aging. Skin, the sirtuin enzymes SIRT1 and SIRT6 — which require NAD+ as a cofactor — both promote collagen production genes and simultaneously suppress MMP-1, the enzyme that degrades collagen. Both SIRT1 and SIRT6 are measurably downregulated in older skin, and this downregulation correlates directly with reduced NAD+ availability.
NAD+ levels in human skin decline with age, and this decline affects multiple repair mechanisms simultaneously: DNA repair capacity (through PARP enzyme activity), mitochondrial energy production in skin cells, autophagy of damaged proteins, including glycated collagen, and the sirtuin-mediated preservation of collagen integrity. Restoring NAD+ doesn’t just address one pathway — it re-enables the entire network of cellular maintenance processes that keep skin in a regenerative rather than senescent state.
For skin rejuvenation, NAD+ IV therapy produces a faster and larger increase in cellular NAD+ than oral supplementation, making it the preferred delivery method in clinical protocols. This is particularly relevant when pairing NAD+ with aesthetic procedures like laser treatments or microneedling — adequate NAD+ levels allow cells to respond more effectively to the controlled damage stimulus that drives collagen remodeling in those procedures.
GHK-Cu (Copper Peptide): Collagen, Elastin, and Topical Repair
GHK-Cu is a naturally occurring copper-binding peptide with one of the strongest topical penetration profiles among skin-active peptides. It promotes fibroblast proliferation, stimulates collagen and elastin synthesis, activates antioxidant defense enzymes, and has documented anti-inflammatory effects. Unlike most of the injectable peptides covered above, GHK-Cu has meaningful evidence for topical application — it’s small enough to cross the stratum corneum and reach dermal fibroblasts at relevant concentrations. It works well as a topical complement to systemic peptide protocols, providing a local signal for collagen synthesis while the injectable peptides address growth hormone levels and cellular aging mechanisms.
How to Implement a Peptide Protocol for Skin Rejuvenation

Before starting any peptide protocol, a clinical consultation and baseline bloodwork are strongly recommended. Foundational biomarker testing establishes hormone levels, inflammatory markers, and other indicators that help determine which peptides are appropriate and at what doses. This isn’t just a safety measure — it gives you a baseline against which to measure whether the protocol is producing the expected changes.
Standard protocols for skin-focused peptide therapy typically run 3 to 4 months, with a rest period afterward. This cycling approach prevents receptor desensitization and gives the body time to consolidate the changes produced during the active phase. Dosing frequency varies by peptide — growth hormone secretagogues are typically administered 2 to 3 times per week, usually in the evening to align with the natural GH pulse; BPC-157 and TB-500 protocols run on a similar frequency.
Most people notice the first changes between weeks 4 and 8 — improved skin texture, reduced dryness, and early firmness improvements. More structural changes like meaningful wrinkle reduction or improved jaw definition take longer, typically 10 to 16 weeks of consistent use. Progress tracking with consistent photos taken under the same lighting conditions makes it easier to assess changes that happen gradually over months rather than days.
Maximizing Peptide Therapy Results for Skin
Peptide protocols produce their best results when the supporting lifestyle conditions are in place. Sleep is the most operationally important one: growth hormone is primarily secreted in the first two hours of slow-wave sleep, so administering CJC-1295/Ipamorelin before bed and maintaining consistent sleep timing directly affects how much GH gets released in response to the peptide signal. Poor sleep quality is one of the most common reasons peptide protocols underperform.
Diet affects collagen synthesis more directly than most people realize. Collagen is built from the amino acids glycine, proline, and hydroxyproline — all of which need to be available from dietary protein. Vitamin C is required for the hydroxylation step that converts proline to hydroxyproline; inadequate vitamin C is a reliable way to limit collagen production regardless of what the signaling environment looks like. Zinc and copper are cofactors for collagen cross-linking enzymes. Getting adequate protein and micronutrients removes a common bottleneck in the collagen production pathway.
Sun exposure is the largest environmental accelerant of skin aging, primarily through UV-driven DNA damage in keratinocytes and free radical generation that degrades collagen. Running a peptide protocol while continuing unprotected sun exposure is working against the protocol’s goals. Daily SPF 30 or higher is baseline, not optional, during an anti-aging peptide program.
Medical aesthetics procedures can be effectively combined with peptide therapy, and the timing matters. PRP facials work through a mechanism — concentrated growth factors stimulating fibroblast activity — that is complementary to what growth hormone secretagogues and BPC-157 do systemically. Running these together produces better outcomes than either alone. Similarly, NAD+ levels should be optimized before laser or microneedling procedures to ensure cells are in a state where they can mount an effective repair response.
Peptide Safety and Best Practices
The peptides covered in this post have generally favorable safety profiles in the existing research literature — BPC-157 has been studied across multiple models with no reported toxicity at typical doses, Epithalon has decades of Eastern European clinical use, and growth hormone secretagogues are better-studied than pharmaceutical GH for safety. That said, ‘generally favorable in research’ is not the same as ‘proven safe for all individuals at all doses’ — a distinction that matters when making clinical decisions.
Known contraindications vary by peptide. Growth hormone secretagogues are not appropriate for people with active cancer or a history of hormone-sensitive tumors, as GH can stimulate cell division broadly. Peptides that activate telomerase (Epithalon) warrant careful consideration in anyone with a personal or family history of cancer for similar reasons. BPC-157 and TB-500 have fewer documented contraindications but should still be used under medical supervision.
Storage and handling significantly affect peptide stability. Most injectable peptides require refrigerated storage, protection from light, and reconstitution with bacteriostatic water using sterile technique. Improperly stored or handled peptides can degrade before use, reducing efficacy or, in some cases, producing unintended effects. The guidance provided with LIVV peptide products includes storage requirements and reconstitution instructions for each peptide.
Monitoring during a peptide cycle is straightforward: track subjective changes (sleep, energy, skin texture), use consistent photographs to document visible changes, and consider follow-up lab work at the end of a cycle to assess whether biomarkers have moved in the expected direction.
LIVV’s Peptide Offerings: Products, Shop, and Consultation
LIVV Natural’s skin health peptide shop carries research-grade peptides including BPC-157, Epithalon, CJC-1295/Ipamorelin, Tesamorelin, TB-500, and GHK-Cu. Products are third-party tested, stored, and shipped under conditions that maintain stability and come with handling and reconstitution guidance. The anti-aging peptide category includes additional options beyond the skin-specific protocols covered here.
LIVV’s medical team is available for consultation to help match specific goals to a protocol — whether the goal is collagen rebuilding, post-procedure recovery, cellular anti-aging, or a combination of the above. Starting from bloodwork rather than a standard menu ensures the protocol fits the individual’s actual hormonal and inflammatory baseline rather than assumptions about what people at a given age typically need.
LIVV Little Italy (800 West Ivy St, Suite A, San Diego, Mon-Fri 9 am-5 pm) and LIVV Cardiff (2027 Newcastle Ave, Cardiff, Tues-Fri 10-6, Sat 10-4, Sun 11-4) both offer in-person consultations. The Cardiff membership additionally provides ongoing protocol management within a structured clinical relationship — relevant for people who want their peptide protocol actively managed alongside other longevity therapies rather than self-administered independently. Full details on what membership includes are on the LIVV Cardiff membership page.
FAQ
How long before peptide therapy produces visible skin changes?
Most people notice the first changes between weeks 4 and 8 — typically improved skin texture, reduced surface dryness, and early firmness. More structural changes like meaningful reductions in wrinkle depth or improved skin laxity take longer, with most protocols requiring 10 to 16 weeks of consistent use before those changes are clearly visible. Growth hormone secretagogue protocols (CJC-1295/Ipamorelin, Tesamorelin) tend to show dermal thickness improvements more gradually than repair-focused peptides like BPC-157, which can produce noticeable healing acceleration within the first few weeks when used in a post-procedure recovery context.
Can peptide therapy replace cosmetic procedures like fillers or laser treatments?
Not exactly — they address different things. Fillers replace lost volume immediately; peptide therapy rebuilds the underlying tissue that produces and maintains that volume over time. Laser treatments stimulate controlled skin damage to trigger repair; peptides like BPC-157 and NAD+ restoration make the repair response to that damage faster and more effective. The most sensible approach combines both: use procedures for immediate results where they make sense, and use peptide protocols to maintain and build on those results. A PRP facial combined with a peptide protocol addressing collagen synthesis will typically produce better long-term outcomes than either approach used in isolation.
What’s the difference between topical peptides and injectable peptides for skin?
The main difference is bioavailability at the target tissue. Most peptides don’t cross the skin barrier in sufficient quantities to produce meaningful effects at dermal fibroblasts — the cells responsible for collagen production. Injectable peptides administered subcutaneously reach systemic circulation and target tissues at therapeutic concentrations. Topical peptides are useful for certain applications (GHK-Cu copper peptide has reasonable evidence for topical activity), but for the major therapeutic peptides — growth hormone secretagogues, BPC-157, Epithalon — systemic delivery is required to produce the effects seen in the research literature.
Are there peptide-specific protocols for different skin concerns?
Yes, and the choice of peptide depends on the primary mechanism driving a person’s skin concerns. Diffuse collagen loss and reduced skin thickness across the face respond best to growth hormone-stimulating peptides (CJC-1295/Ipamorelin or Tesamorelin). Active inflammation, uneven healing, or post-procedure recovery benefit most from BPC-157 and TB-500. Underlying cellular aging — particularly in people noticing accelerated changes despite good lifestyle habits — warrants Epithalon and NAD+ to address the telomere and sirtuin pathways. Most people benefit from a combination protocol rather than a single peptide, and a clinical consultation is the most efficient way to match the protocol to the actual concern.
How do I know if a peptide protocol is working?
Consistent photography under the same lighting conditions is the most practical tracking method — changes that happen over months are difficult to perceive day-to-day but clearly visible in before-and-after comparisons taken 8 weeks apart. Subjective markers — sleep quality, energy levels, skin texture on touch, and how quickly minor skin damage heals — are also useful early indicators. For people using growth hormone secretagogues, lab markers, including IGF-1 levels, can provide objective confirmation that the protocol is producing the expected hormonal response. A follow-up biomarker panel at the end of a 3 to 4-month cycle gives objective data that the protocol is moving the right numbers, which is more informative than any subjective assessment.
Explore LIVV’s Peptide Products or Schedule a Consultation
If you’re ready to move beyond surface-level skincare, LIVV’s peptide therapy overview covers the full scope of what’s available. The skin health and anti-aging peptide categories in the LIVV shop carry research-grade products with the storage and handling standards that clinical-grade protocols require. For people who want a protocol matched to their specific lab data and goals rather than a standard selection, clinical consultations are available at both LIVV locations and can be booked through the LIVV website.
For context on how peptide therapy fits into a broader anti-aging approach, the LIVV blog covers the latest anti-aging protocols and how to reverse aging at the biological level — both of which situate peptide therapy within the wider framework of cellular and hormonal interventions that make up a complete longevity protocol.